

Anticipation
Seeing what you want to see

Information now usually comes in a visual, not textual form. The internet has made it so, and we humans, eyes-first predators, are quick to shed our reliance on reading.
But we don’t get much training in how to see.
Notice anything?
This is an example of how we evaluate the visual world. This specific example comes from an article I read many years ago, one that has occupied a central place in my personal learning of pathology. (It is not, I should note, what is taught to pathology trainees.) In this article from 2006, Dr. McLendon, a neuropathologist, wrote about what can be learned about cognitive processes of decision making by studying how CIA analysts process information to make decisions.* Just like in pathology, CIA analysts must take in information that is incomplete and ambiguous and make important decisions.
One way to examine how this is done is to consider these optical illusions that highlight cognitive biases.
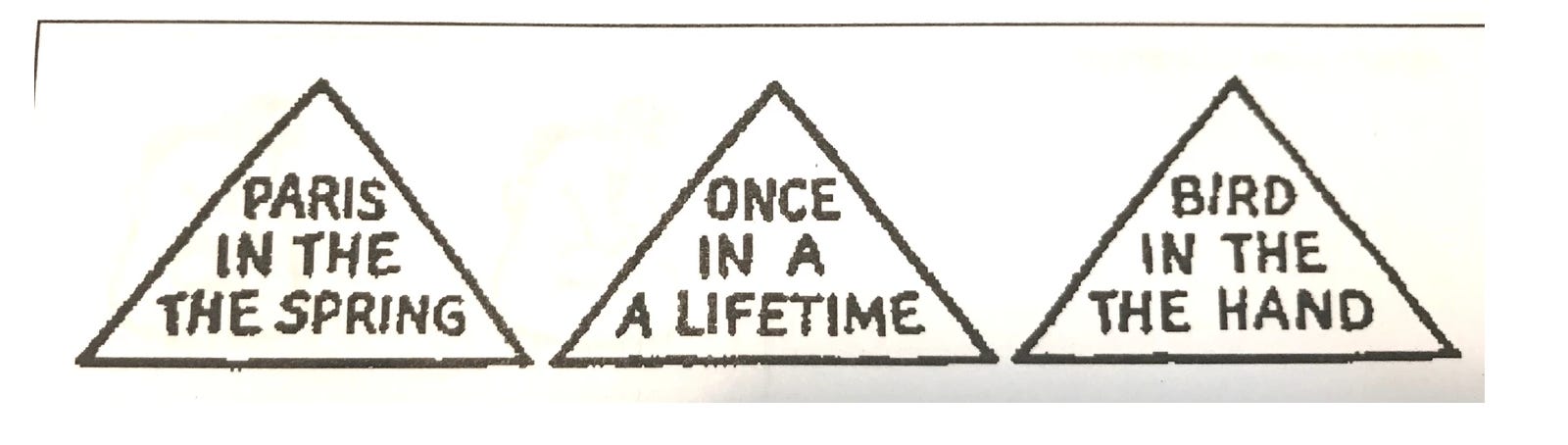
Reading over the pyramids again:
Paris in the the spring Once in a a lifetime Bird in the the hand
One Monday morning, as a surgical pathology fellow, I was reviewing an appendix. It had been removed over the weekend, and the pathologist and I were going over the cases that had accumulated before we started getting the morning specimens from the ORs. Like most of the weekend specimens, this was an unexpected surgery. It was performed on a patient who came in for emergency appendicitis. I took the slide from the histology technician, laid it on my microscope stage, and examined it. I looked for the hallmark of this condition - acute inflammation, or neutrophils, through the full wall thickness of the appendix. I found that feature and was done with my examination.
"Appendicitis," I said, quickly handing the slide to the attending pathologist, my superior.
She then looked at the slide and within a moment had stood up to go look at the specimen on the gross station. She sat back down next to me.
"Jena, " she said, "if you only look for appendicitis, that's all you will ever see."
The specimen contained an appendiceal carcinoma. Acute appendicitis was in fact present - but only as a secondary phenomenon.
The main reason why pathologists even examine the appendix is to ensure this carcinoma is not overlooked. And I had done so. That moment burned a hole of shame in my vision that still lingers. I had anticipated the answer and so that anticipation dictated what I would see. A lesson I'll never forget.
Fear and humility are not necessarily bad teachers. Lessons learned during medical training generate a reference library of differential diagnoses. The differential diagnosis is a list of possible explanations for a given condition, and it guides the tests needed to disprove and prove each of these, in order to arrive at the correct diagnosis.
The process by which pathologists develop differential diagnoses lists is frighteningly subjective and often harrowing - it is uncomfortable to talk about these aspects of pathology training, However, it is important to consider because it is not just pathologists and CIA analysts who are taking in incomplete information.
No one is teaching the general public to hone their perceptive skills in looking at the world on the internet, to develop lists of possible explanations and not leap to an intuitive explanation. All of us imperfectly perceive reality, form an opinion, and make a decision. We are often unaware of what we are anticipating in any encounter, leading us to an inaccurate assessment. All too often we are only seeing what we look for, and missing the big picture in the process.
Arch Pathol Lab Med (2006) 130 (5): 613–616.